Maternal sepsis deaths in sub-Saharan Africa dwarf Europe
WaterAid links fatality gap to missing water sanitation and hygiene in maternity wards, the cheapest fixes are taps toilets and soap
Images
 WaterAid
WaterAid
 WaterAid
WaterAid
 Miatta Kromah holding the hand of her baby girl after delivering her at Diah Clinic, Grand Cape Mount, Liberia (Cianeh Kpukuyou/WaterAid)
Cianeh Kpukuyou/WaterAid
Miatta Kromah holding the hand of her baby girl after delivering her at Diah Clinic, Grand Cape Mount, Liberia (Cianeh Kpukuyou/WaterAid)
Cianeh Kpukuyou/WaterAid
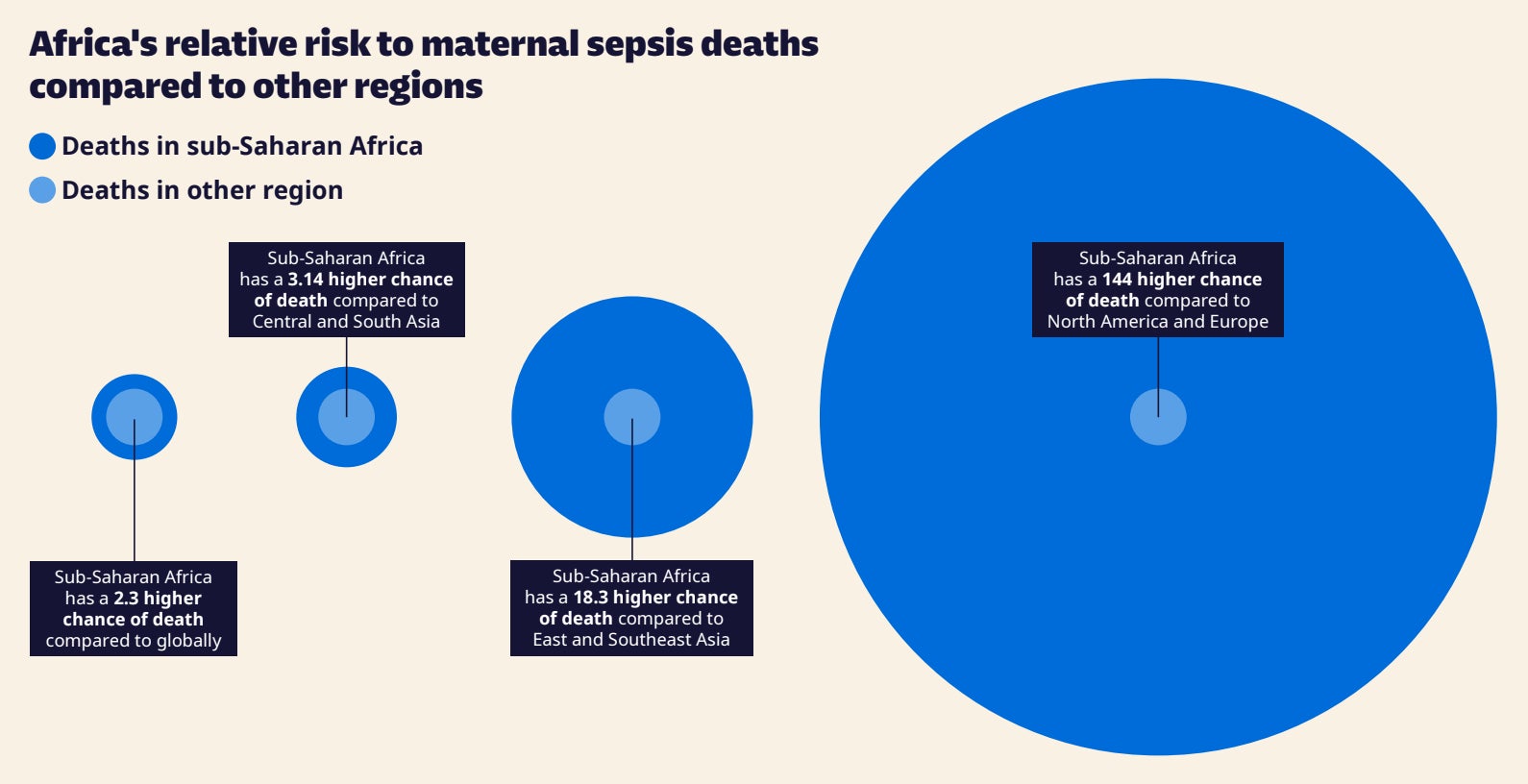
Women who develop maternal sepsis in sub‑Saharan Africa are almost 150 times more likely to die than mothers in Britain, Europe and North America, according to a WaterAid analysis cited by The Independent. The charity estimates 4.7 million women in the region develop maternal sepsis each year—about one in nine births—and reports that the condition contributes to roughly 36 deaths a day, with facilities often lacking clean water, toilets and basic hygiene.
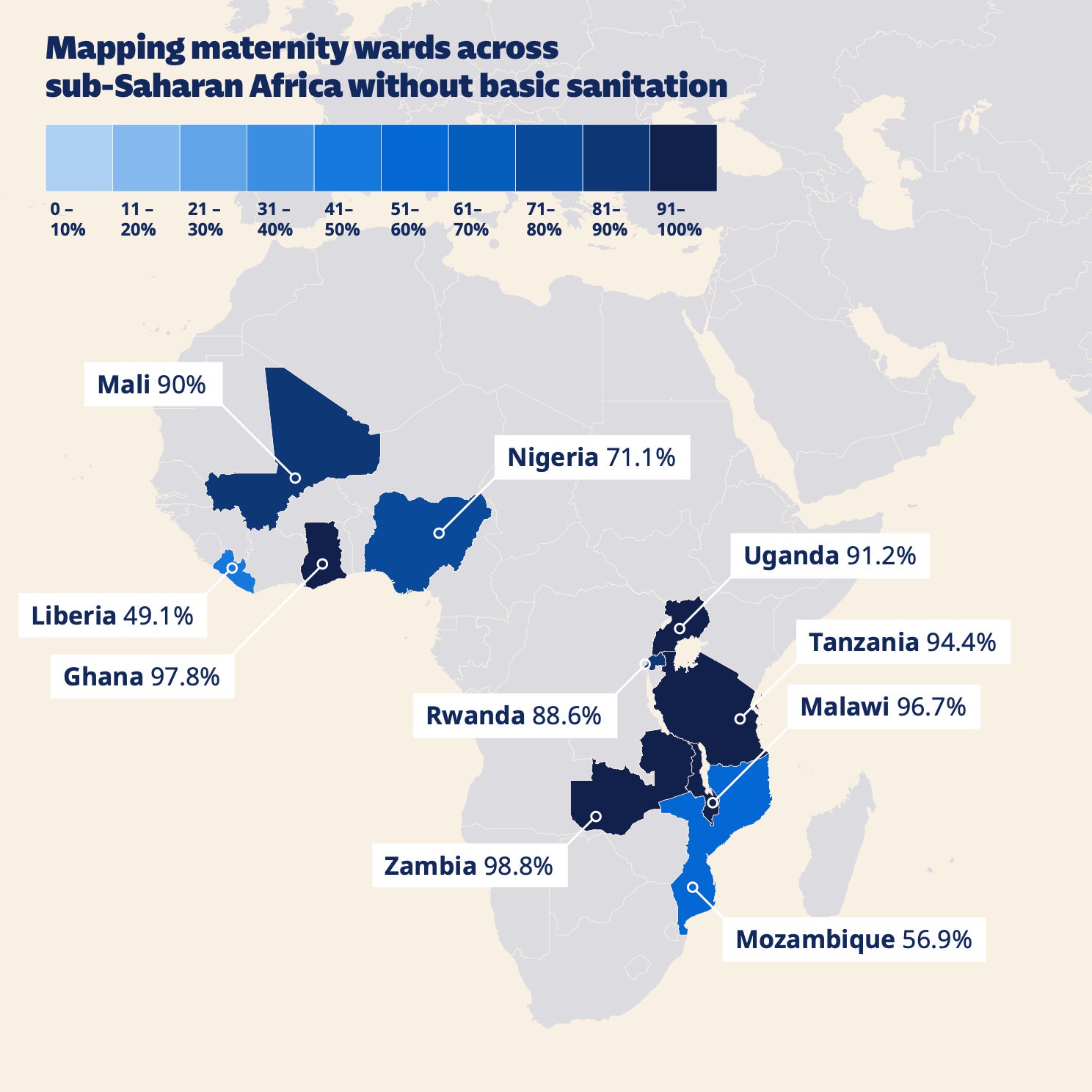
The gap is often discussed as a problem of “awareness” or clinical training, but the chain that produces sepsis is stubbornly physical. Infection risk rises when births take place in crowded wards where staff cannot reliably wash hands, clean surfaces, or dispose of waste; when mothers arrive late after prolonged labour; and when basic diagnostics and first-line antibiotics are delayed or unavailable. WaterAid’s survey across 16 countries in Africa and Asia found that, in the African facilities assessed, 78% lacked a functioning toilet, two‑thirds lacked clean water and soap for handwashing, and 65% did not meet basic environmental cleaning standards.
Those numbers matter because the earliest, cheapest breaks in the chain are not intensive-care technologies but mundane infrastructure. If a ward has running water, soap, and a workable toilet, the baseline bacterial load in the environment falls; staff compliance becomes feasible rather than aspirational; and routine procedures—vaginal examinations, caesarean sections, catheter use—carry less contamination risk. Once infection is established, speed becomes the scarce resource: triage that recognises danger signs, access to IV antibiotics, and the ability to monitor and escalate care. Where those steps fail, ICU capacity becomes the last bottleneck, but by then the patient is already expensive to save.
WaterAid argues that water, sanitation and hygiene (WASH) investment in health facilities could prevent about 10 million maternal sepsis cases and 8,580 deaths globally each year at a cost of less than $1 per person. That estimate is necessarily model-driven, but it clarifies what is being purchased: fewer infections to treat, not merely better treatment of infections that have already spread. It also sits uneasily alongside the reality that many clinics still operate without the inputs that make modern obstetrics safe.
The report arrives as aid budgets are under pressure in both the US and UK, which WaterAid says threatens WASH upgrades in maternity care. A system that cannot fund taps, toilets and soap is unlikely to fund the antibiotics, lab capacity and staffed high-dependency beds that sepsis treatment ultimately requires.
In WaterAid’s accounting, three out of four facility births in sub‑Saharan Africa take place without adequate water, sanitation or hygiene. The intervention begins with plumbing.